
History
A 2-year-old dog, weighing 7.6 kg, was rescued after being abandoned at a lodge. According to the previous owners, the dog had liver abnormalities and had a specialized diet. Blood tests revealed alterations in bile acids and alanine transaminase (ALT) levels. An abdominal ultrasound suggested a possible portosystemic shunt. Surgery was attempted, however, failed to find the anomaly. An abdominal CT angiography (CTA) was requested to identify the suspected anomalous vessel.
Diagnosis
CTA images showed a large anomalous vessel, arising from the portal vein, following a tortuous path cranially along the lesser curvature of the stomach, reaching the cranial pole of the right kidney and finally draining into the caudal vena cava. The anomalous vessel measured approximately 11 mm in diameter at its origin and 7 mm immediately before its insertion. Both the portal veins and the vena cava were dilated. An extrahepatic portocaval shunt, at the level of the gastroduodenal transition, was diagnosed. Subsequently, the dog underwent surgical treatment and recovered well.

Fig. 1: Oblique views of a transversal image (Fig. 1a) and a MIP image (Fig. 1b), as well as an image in median plane (Fig. 1c) show a large anomalous vessel, arising from the portal vein (arrows) and draining into the caudal vena cava (dotted arrows).
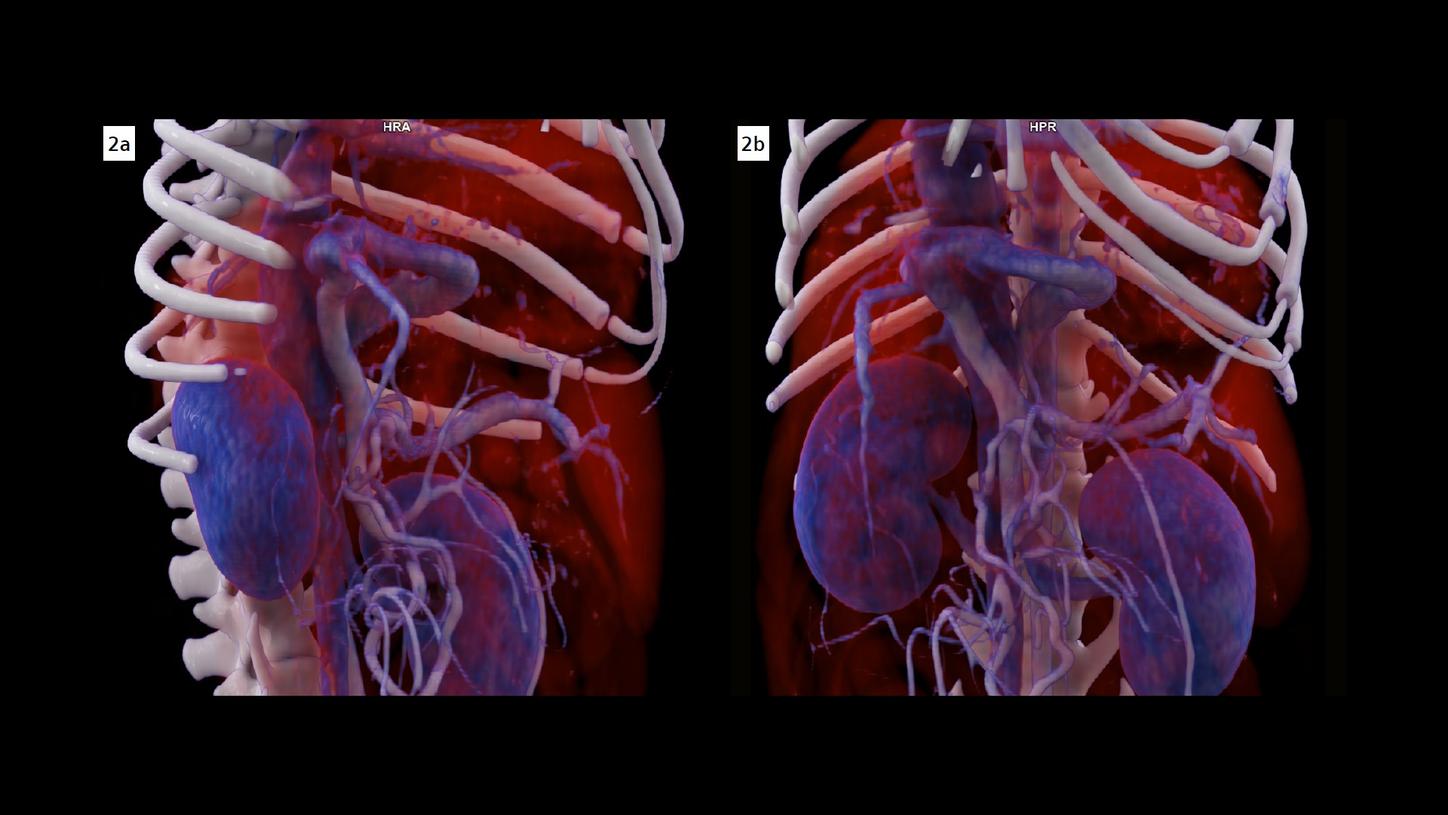
Fig. 2: Two VRT images show the origin, the course and the draining location of the portocaval shunt in three dimensions.
Comments
A portosystemic shunt is an anomalous vascular connection between the portal venous system and the systemic circulation. It is usually connected to the caudal vena cava, then called a portocaval shunt, or to the azygous vein. Connection to other systemic vessels is rare. This anomaly, which can be congenital or acquired, intrahepatic or extrahepatic, occurs in animals, particularly in dogs. The shunt allows blood to bypass the hepatic portal system, crippling the liver’s ability to process toxins and maintain metabolic homeostasis, resulting in serious health consequences. Surgical treatment, aiming at occluding the shunt and restoring normal hepatic blood flow, is definitive. However, a surgical attempt can fail without the help of a precise pre-operative planning based on an accurate localization of the shunt and a clear visualization of its course. In veterinary medicine, CT imaging has become a preferred diagnostic method. CT images can be reconstructed and visualized in transversal, dorsal and median planes with no overlapping of different anatomical structures. A three-dimensional, lifelike demonstration, using cinematic volume rendering technique (cVRT), facilitates the communication with the surgeons. As shown in this case, with a clear visualization of the shunt, the second surgery was successful.
Examination Protocol